
UMN vs LMN refers to the difference between upper motor neuron and lower motor neuron lesions. Upper motor neuron lesions cause spasticity, hyperreflexia, and increased muscle tone, while lower motor neuron lesions cause flaccid paralysis, muscle wasting, and reduced reflexes. Understanding UMN vs LMN is essential for diagnosing stroke, spinal cord injury, and peripheral nerve disorders.
When a patient has weakness, doctors ask one key question. Is it UMN vs LMN?
This simple difference can change the diagnosis. It can point to a stroke. It can show a spinal cord injury. It can even reveal a nerve problem.
Upper motor neurons and lower motor neurons work together to control movement. If one part is damaged, the body reacts in a specific way. The signs are not random. They follow clear patterns.
Many students feel confused about UMN vs LMN. The symptoms seem similar at first. Both can cause weakness. Both affect movement. But the reflexes, muscle tone, and muscle size tell a different story.
This article explains UMN vs LMN in a simple way. You will learn definitions, examples, comparison tables, common mistakes, and practice questions. By the end, you will confidently identify the difference between upper and lower motor neuron lesions in real clinical cases.
Quick Answer About UMN vs LMN
UMN vs LMN can be summarized in one table:
| Feature | Upper Motor Neuron (UMN) Lesion | Lower Motor Neuron (LMN) Lesion |
|---|---|---|
| Muscle Tone | Increased (Spastic) | Decreased (Flaccid) |
| Reflexes | Hyperreflexia | Hyporeflexia or Areflexia |
| Muscle Wasting | Mild | Severe |
| Fasciculations | Absent | Present |
| Babinski Sign | Positive | Negative |
| Paralysis Type | Spastic | Flaccid |
In short:
- UMN lesion = stiff muscles and strong reflexes
- LMN lesion = floppy muscles and weak reflexes
What Are Upper Motor Neurons
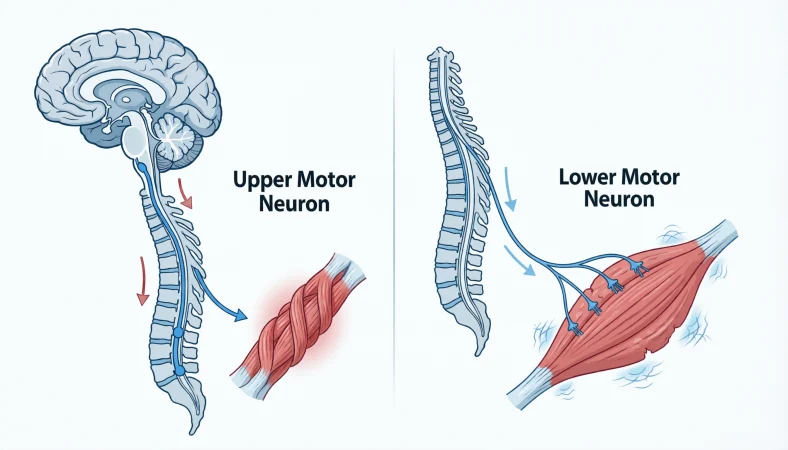
Upper motor neurons begin in the motor cortex of the brain. They travel down through the brainstem and spinal cord.
Their main pathway is called the corticospinal tract.
Upper motor neurons do not directly touch muscles. Instead, they send signals to lower motor neurons.
Think of UMN as managers in an office. They give instructions but do not do the physical work.
If upper motor neurons are damaged, control is lost. The lower motor neurons become overactive. This leads to spasticity and exaggerated reflexes.
Common causes of UMN lesions:
- Stroke
- Brain tumor
- Multiple sclerosis
- Spinal cord injury above anterior horn
What Are Lower Motor Neurons
Lower motor neurons begin in the anterior horn of the spinal cord or in cranial nerve nuclei.
They travel directly to the muscle.
LMNs are the final pathway for movement. Without them, muscles cannot contract.
Think of LMN as workers in the office. They do the actual job.
When LMNs are damaged, the muscle loses its direct nerve supply. The muscle becomes weak, floppy, and eventually shrinks.
Common causes of LMN lesions:
- Peripheral nerve injury
- Polio
- Radiculopathy
- Guillain Barre syndrome
- Amyotrophic lateral sclerosis involving LMN component
Understanding the Pathway in UMN vs LMN
To fully understand UMN vs LMN, you must know the movement pathway.
- Brain motor cortex starts the signal
- Upper motor neuron carries signal down
- It synapses in spinal cord
- Lower motor neuron carries signal to muscle
- Muscle contracts
Damage location determines the signs.
If damage is above the synapse → UMN signs
If damage is at or below the synapse → LMN signs
Detailed Comparison of UMN vs LMN
Muscle Tone
- UMN lesion increases tone
- LMN lesion decreases tone
Spasticity means tight resistance during passive movement. It is velocity dependent.
Flaccidity means loose and soft muscle.
Reflexes
In UMN lesion:
- Reflex arc remains intact
- Brain inhibition is lost
- Reflex becomes exaggerated
In LMN lesion:
- Reflex arc is broken
- Reflex is reduced or absent
Muscle Bulk
- UMN lesion causes mild disuse atrophy
- LMN lesion causes severe neurogenic atrophy
Fasciculations
Small visible muscle twitches occur in LMN lesions because damaged neurons fire randomly.
They do not occur in pure UMN lesions.
Advantages and Disadvantages of Recognizing UMN vs LMN Early
Advantages
- Faster stroke diagnosis
- Better localization of spinal cord injury
- Early treatment of nerve disorders
- Improved rehabilitation planning
Disadvantages of Misdiagnosis
- Wrong imaging area
- Delayed treatment
- Unnecessary tests
- Poor outcome
Correctly identifying UMN vs LMN saves time and improves patient care.
Real World Examples of UMN vs LMN
Stroke Patient
A 65 year old man develops sudden right sided weakness.
Findings:
- Increased tone
- Hyperreflexia
- Positive Babinski
This is UMN lesion. Likely stroke affecting motor cortex.
Peripheral Nerve Injury
A man cuts his wrist and cannot extend his fingers.
Findings:
- Flaccid weakness
- Reduced reflex
- Muscle wasting over time
This is LMN lesion.
Spinal Cord Injury
If injury is above L1:
- UMN signs in legs
- Possible LMN signs at injury level
This mixed pattern helps localize lesion.
Regional and Global Usage of UMN vs LMN Diagnosis
Across the world, neurological examination relies on UMN vs LMN principles.
In emergency rooms in the United States, Europe, Asia, and Africa, doctors use reflex testing and tone assessment to localize lesions.
In low resource settings, physical examination is even more important because imaging may not be immediately available.
Thus, understanding UMN vs LMN is a universal medical skill.
Common Mistakes in UMN vs LMN Identification
Mistake 1: Thinking all weakness is LMN
Correction: Check reflexes and tone first.
Mistake 2: Ignoring Babinski sign
Babinski is a strong UMN indicator.
Mistake 3: Confusing early spinal shock
Immediately after spinal cord injury:
- Reflexes may be absent
- Muscles may be flaccid
This looks like LMN but later becomes UMN pattern.
Mistake 4: Forgetting mixed lesions
Some diseases like ALS show both UMN and LMN signs.
Related Concepts in UMN vs LMN
Spastic vs Flaccid Paralysis
Spastic = UMN
Flaccid = LMN
Babinski Reflex
Upgoing plantar response indicates UMN lesion.
Clonus
Rhythmic muscle contraction seen in UMN lesion.
Motor Unit
LMN plus its muscle fibers form a motor unit.
UMN vs LMN in Advanced Clinical Context
Amyotrophic Lateral Sclerosis
ALS affects both upper and lower motor neurons.
Signs:
- Spasticity
- Hyperreflexia
- Fasciculations
- Muscle wasting
Mixed pattern confirms dual involvement.
Multiple Sclerosis
Often causes UMN lesions due to demyelination in CNS.
Diabetic Neuropathy
Causes LMN pattern due to peripheral nerve damage.
Clinical Examination Steps in UMN vs LMN
- Inspect muscle bulk
- Look for fasciculations
- Test tone
- Check reflexes
- Test plantar response
These five steps solve most UMN vs LMN questions.
Exercises With Answers
Exercise 1
A patient has hyperreflexia and increased tone. What type of lesion?
Answer: UMN lesion.
Exercise 2
A patient has muscle wasting and fasciculations. Diagnosis?
Answer: LMN lesion.
Exercise 3
Positive Babinski indicates?
Answer: Upper motor neuron lesion.
Exercise 4
Absent reflex with flaccid paralysis suggests?
Answer: Lower motor neuron lesion.
Exercise 5
Spinal cord injury initially causes flaccidity. Later becomes?
Answer: UMN pattern due to loss of inhibition.
Expanded Comparison Table
| Category | UMN Lesion | LMN Lesion |
|---|---|---|
| Location | Brain or spinal cord above anterior horn | Anterior horn, root, nerve |
| Tone | Increased | Decreased |
| Reflex | Increased | Decreased |
| Atrophy | Mild | Severe |
| Fasciculation | No | Yes |
| Babinski | Positive | Negative |
| Clonus | Present | Absent |
FAQs
What is the main difference between UMN vs LMN?
UMN lesions cause spasticity and hyperreflexia, while LMN lesions cause flaccidity and muscle wasting.
How do you quickly identify UMN vs LMN in exam?
Check tone and reflexes first. Increased tone and reflexes suggest UMN. Decreased suggest LMN.
Can a disease show both UMN and LMN signs?
Yes. ALS shows mixed upper and lower motor neuron involvement.
Why does UMN lesion cause hyperreflexia?
Because brain inhibition over reflex arc is lost.
Why does LMN lesion cause muscle atrophy?
Because muscle loses direct nerve supply.
Is Babinski seen in LMN lesion?
No. Babinski is a classic UMN sign.
Does stroke cause UMN or LMN pattern?
Stroke typically causes UMN pattern.
Can spinal cord injury cause LMN signs?
At the level of injury yes. Below the level usually UMN signs.
Is fasciculation seen in UMN vs LMN comparison?
Fasciculations are seen in LMN lesions.
Why is understanding UMN vs LMN important?
It helps localize neurological damage quickly and accurately.
Conclusion
Understanding UMN vs LMN is one of the most important skills in neurology. It helps doctors localize damage in the brain, spinal cord, or peripheral nerves. The key differences involve muscle tone, reflexes, muscle bulk, and pathological signs like Babinski.
Remember the core rule. Spastic and hyperreflexic means UMN. Flaccid and hyporeflexic means LMN.
Use a systematic examination approach. Inspect, feel tone, check reflexes, and test plantar response. Avoid common mistakes like confusing early spinal shock with LMN lesion.
For students, practice using clinical cases. For professionals, always confirm findings with imaging when needed.
Mastering UMN vs LMN improves diagnosis speed, treatment accuracy, and patient outcomes


