Last Updated on May 19, 2026
AVNRT vs AVRT are two common types of supraventricular tachycardia caused by different electrical reentry circuits in the heart. AVNRT occurs within or near the AV node, while AVRT involves an extra electrical pathway between the atria and ventricles. Understanding the difference helps in correct diagnosis and treatment.
AVNRT vs AVRT is a topic that often confuses students, patients, and even new clinicians. Both conditions cause fast heartbeats that start suddenly and stop suddenly. They may feel the same to a patient, but inside the heart, the causes are very different.
These two arrhythmias are types of supraventricular tachycardia. That means the fast rhythm starts above the ventricles. AVNRT comes from a reentry loop inside the AV node. AVRT happens when an extra electrical pathway connects the atria and ventricles.
Why does this matter? Because treatment and ECG patterns can change based on the type. Wrong identification can lead to wrong management choices in some cases.
In this article, we will explain AVNRT vs AVRT in very simple language. You will learn how to tell them apart, how they behave on ECG, how doctors diagnose them, and how they are treated. This guide is useful for medical students, healthcare workers, and anyone trying to understand heart rhythm problems clearly.
Quick Answer Overview
AVNRT vs AVRT difference in simple terms:
AVNRT is a reentry rhythm inside the AV node itself. AVRT uses an accessory pathway outside the AV node to create a loop. AVNRT usually has no extra pathway, while AVRT is strongly linked with conditions like Wolff Parkinson White syndrome.
Both cause fast heart rate, palpitations, dizziness, and chest discomfort. However, their ECG patterns and treatment strategies can differ.
Definition of AVNRT vs AVRT
What is AVNRT?
AVNRT stands for Atrioventricular Nodal Reentrant Tachycardia. It is a type of fast heart rhythm caused by a small reentry circuit inside or near the AV node.
The AV node normally controls electrical signals between atria and ventricles. In AVNRT, the signal gets trapped in a loop using two pathways within the AV node.
This causes rapid and regular heartbeats, often between 140 to 250 beats per minute.
What is AVRT?
AVRT stands for Atrioventricular Reentrant Tachycardia. It is also a reentry rhythm, but it involves an extra electrical connection between the atria and ventricles.
This extra connection is called an accessory pathway. It allows electricity to bypass the AV node and form a loop.
The most common condition linked to AVRT is Wolff Parkinson White syndrome.
Mechanism of AVNRT vs AVRT
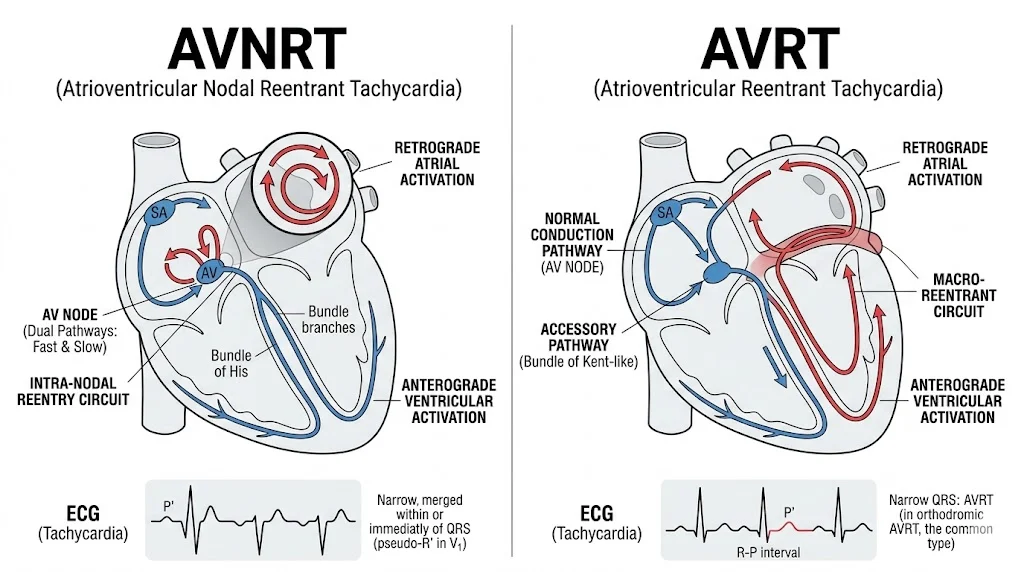
Mechanism of AVNRT
In AVNRT, there are two pathways inside or near the AV node:
- Slow pathway
- Fast pathway
A premature heartbeat can trigger a loop:
- Electrical impulse goes down the slow pathway.
- It returns up through the fast pathway.
- A continuous loop forms.
- Heart rate becomes very fast.
This is why AVNRT is called a “nodal reentry.”
Mechanism of AVRT
In AVRT, the mechanism involves two separate structures:
- AV node
- Accessory pathway (extra electrical bridge)
The loop works like this:
- Signal goes from atria to ventricles through AV node.
- It returns to atria through accessory pathway.
- A circular loop continues.
This creates a “macro reentry circuit,” which is larger than AVNRT.
AVNRT vs AVRT Comparison Table
| Feature | AVNRT | AVRT |
| Full form | Atrioventricular Nodal Reentrant Tachycardia | Atrioventricular Reentrant Tachycardia |
| Location | AV node | AV node + accessory pathway |
| Extra pathway | No | Yes |
| Common association | No structural disease | Wolff Parkinson White syndrome |
| ECG P waves | Often hidden | May be visible or abnormal |
| RP interval | Short | Often longer |
| Mechanism size | Small circuit | Larger circuit |
| Onset/offset | Sudden | Sudden |
| Most common SVT | Yes | Less common than AVNRT |
Symptoms of AVNRT vs AVRT
Both conditions share similar symptoms because both cause fast heart rates.
Common symptoms include:
- Sudden palpitations
- Chest discomfort
- Shortness of breath
- Dizziness
- Anxiety feeling
- Neck pulsations
- Fatigue after episode
In AVNRT, symptoms often feel very regular and stable.
In AVRT, symptoms may sometimes feel slightly more irregular depending on pathway conduction.
Diagnosis of AVNRT vs AVRT
ECG (Electrocardiogram)
ECG is the most important tool.
In AVNRT:
- Narrow QRS complex
- P waves often hidden inside QRS
- Very regular rhythm
In AVRT:
- May show delta wave in baseline ECG (WPW cases)
- P waves may appear after QRS
- Wider QRS in some cases
Other tests
- Holter monitor
- Event recorder
- Electrophysiology study (EPS)
EPS is the most accurate test to confirm AVNRT vs AVRT.
Advantages and Disadvantages (Clinical Perspective)
This section is about understanding clinical behavior.
AVNRT
Advantages:
- Usually not life-threatening
- Responds well to simple treatments like vagal maneuvers
Disadvantages:
- Can be recurrent
- May affect quality of life
AVRT
Advantages:
- Curable with catheter ablation in many cases
Disadvantages:
- Can be associated with WPW, which may cause serious arrhythmias
- Higher risk in rare cases of fast conduction to ventricles
Treatment of AVNRT vs AVRT
Immediate Treatment
Both conditions initially respond to similar methods:
- Vagal maneuvers (coughing, Valsalva)
- Adenosine injection
- Beta blockers
- Calcium channel blockers
Long-term Treatment
AVNRT Treatment
- Medication control in mild cases
- Catheter ablation of slow pathway in recurrent cases
AVRT Treatment
- Catheter ablation of accessory pathway
- Avoid AV node blocking drugs in WPW with atrial fibrillation
Ablation is highly effective for both conditions.
Real-World Examples of AVNRT vs AVRT
Example of AVNRT
A 25-year-old woman suddenly feels rapid heartbeat while resting. ECG shows narrow complex tachycardia. Valsalva maneuver stops it. Diagnosis: AVNRT.
Example of AVRT
A 30-year-old man with known Wolff Parkinson White syndrome experiences sudden palpitations during exercise. ECG shows abnormal delta wave during normal rhythm. Diagnosis: AVRT.
Global Clinical Practice
AVNRT vs AVRT is studied worldwide in cardiology training.
- AVNRT is the most common SVT seen in emergency rooms.
- AVRT is more commonly linked with electrophysiology labs due to WPW evaluation.
In both developed and developing countries, catheter ablation has become the standard curative approach.
Common Mistakes in AVNRT vs AVRT Understanding
Many learners confuse these conditions.
Common mistakes include:
- Thinking all SVT is AVNRT
- Assuming AVRT always shows WPW pattern on ECG
- Misreading P waves in tachycardia
- Confusing wide QRS AVRT with ventricular tachycardia
- Ignoring clinical history of sudden onset and offset
Correct understanding requires ECG practice and EP study knowledge.
Exercises with Answers
Exercise 1
A patient has sudden narrow complex tachycardia. No delta wave is seen in baseline ECG. Most likely diagnosis?
Answer: AVNRT
Exercise 2
Which condition involves an accessory pathway?
Answer: AVRT
Exercise 3
True or False: AVNRT requires an extra electrical pathway outside the AV node.
Answer: False
Exercise 4
What is the first-line acute treatment for both AVNRT vs AVRT?
Answer: Vagal maneuvers or adenosine
Exercise 5
Which condition is most associated with Wolff Parkinson White syndrome?
Answer: AVRT
Related Concepts and Comparisons
AVNRT vs AVRT vs WPW
- AVNRT: AV node circuit only
- AVRT: involves accessory pathway
- WPW: condition that often leads to AVRT
AVNRT vs Atrial Fibrillation
- AVNRT is regular rhythm
- AF is irregular rhythm
AVRT vs Ventricular Tachycardia
- AVRT is supraventricular
- VT originates in ventricles and is more dangerous
FAQs
What is the main difference between AVNRT vs AVRT?
AVNRT occurs inside the AV node, while AVRT uses an accessory pathway outside the AV node.
Is AVNRT dangerous?
AVNRT is usually not life-threatening but can be uncomfortable and recurrent.
Can AVRT turn into something serious?
Yes, especially if associated with WPW and atrial fibrillation.
How do doctors confirm AVNRT vs AVRT?
Through ECG, Holter monitoring, and electrophysiology study.
Is catheter ablation effective?
Yes, it is highly effective for both AVNRT and AVRT.
Can lifestyle changes cure AVNRT or AVRT?
No, but they may reduce triggers like stress or caffeine.
Why is AVNRT more common than AVRT?
Because AV node dual pathways are more common than accessory pathways.
Can both conditions happen in young people?
Yes, both often affect young adults.
Do both cause sudden heartbeat episodes?
Yes, both start and stop suddenly.
What is the first emergency treatment?
Vagal maneuvers followed by adenosine if needed.
Conclusion
Understanding AVNRT vs AVRT is essential for recognizing and managing supraventricular tachycardia correctly. Although both conditions cause similar symptoms like palpitations and fast heart rate, their internal mechanisms are very different.
AVNRT is a small reentry circuit within the AV node. AVRT involves an accessory pathway connecting atria and ventricles. This difference affects ECG patterns, diagnosis, and treatment decisions.
Both conditions respond well to acute treatment like vagal maneuvers and adenosine. For long-term cure, catheter ablation is highly effective and widely used.
For learners and healthcare professionals, mastering AVNRT vs AVRT improves ECG interpretation skills and patient care. Always consider clinical history, ECG patterns, and electrophysiology findings together for accurate diagnosis.